








































MACPAC report on Medicaid touts DSRIP, warns about behavioral and dental health
Areas of need for the 71 million person health plan show opportunities for healthcare providers.


As the 50th anniversary of Medicaid approaches, a new report claims there is much work to do on the state-federal program, from finding sustainable hospital payment reforms to tackling the problem of poor oral health.
As the 50th anniversary of Medicaid approaches, a new report claims there is much work to do on the state-federal program, from finding sustainable hospital payment reforms to tackling the problem of poor oral health, according to the Medicaid and CHIP Payment and Access Commission, or MACPAC.
But it is the five-year-old Delivery System Reform Incentive Payments program that ranked highest In MACPAC’s annual report to Congress on the progress and problems in Medicaid.
Authorized under Section 115 waivers, the DSRIP program supports provider-led efforts to reform Medicaid care and promote population health. About $30 billion has been dedicated to DSRIP programs across seven states, including California, Massachusetts, New York and Texas, with payments linked to specific achievements, such as quality reporting or, more ambitiously, outcomes of Medicaid patients. More than 70 million patients are covered under Medicaid or CHIP.
“The DSRIP approach, if taken to scale, has the potential to fundamentally change Medicaid’s role from financing medical care to driving system change toward value and improved health outcomes,” wrote MACPAC chair by Diane Rowland, who is also executive vice president of the Henry J. Kaiser Family Foundation.
However, DSRIP is at a juncture, facing a disconnect in how states and local hospitals and the federal Centers for Medicare & Medicaid Services see it. “Although CMS describes DSRIP programs as a tool primarily intended to assist states in transforming their delivery systems in order to fundamentally improve care for beneficiaries, states have been candid that DSRIP programs have been pursued as a means to make supplemental payments,” MACPAC wrote.
Some states have embraced the DSRIP program. In New York for instance, the program part of the state’s effort to reduce avoidable admissions in Medicaid populations by 25 percent, while ensuring beneficiaries’ access to integrated medical and behavioral health services across primary care practitioners, community-based organizations, home health visits, specialists and hospitals, through “a single system of effective care management.”
[Also: Promise and peril in Medicaid redesign]
To get there, according to MACPAC, states and their hospital partners have to tackle infrastructure development, to expand primary care clinics, mobile health teams and telehealth; and care redesign, such as patient-centered medical home models, co-located behavioral health and primary care, or patient navigator programs.
But MACPAC told Congress that it is only a matter of time before DSRIP goes in reform. “It is challenging to evaluate these programs, and results are not yet available,” MACPAC wrote.
Behavioral health
Medicaid is the nation’s single largest payer for behavioral health services, including mental health and substance use services, accounting for around a quarter of spending, according to MACPAC. And behavioral health conditions also impact a large proportion of adults on Medicaid and children on CHIP, ranging from attention deficit hyperactivity disorder to depression to addiction to schizophrenia.
In 2011, 20 percent of Medicaid beneficiaries had behavioral health diagnoses, and they accounted for almost half of total Medicaid expenditures, with more than $131 billion spent on all of their care. Around 3 million children who qualify for Medicaid based on disability of child welfare assistance had behavioral health diagnosis and accounted for 25 percent of Medicaid spending on children.
Medicaid beneficiaries who are eligible for reasons other than disability have unmet needs for behavioral health screening, treatment and referrals, MACPAC told Congress. “Early intervention and treatment could help delay or prevent loss of function and allow beneficiaries to manage problems before they become disabling,” the Commission said.
[Also: CMS proposes changes to Medicaid managed care, targets rate setting]
“Although severely mentally ill beneficiaries enrolled on the basis of disability incur the highest cost per person, they comprise a relatively small share of total enrollees. On the other hand, many Medicaid beneficiaries enrolled on a basis other than disability may nevertheless be in need of behavioral health screening, treatment and referral; more specialized services would help them delay or prevent future loss of function.”
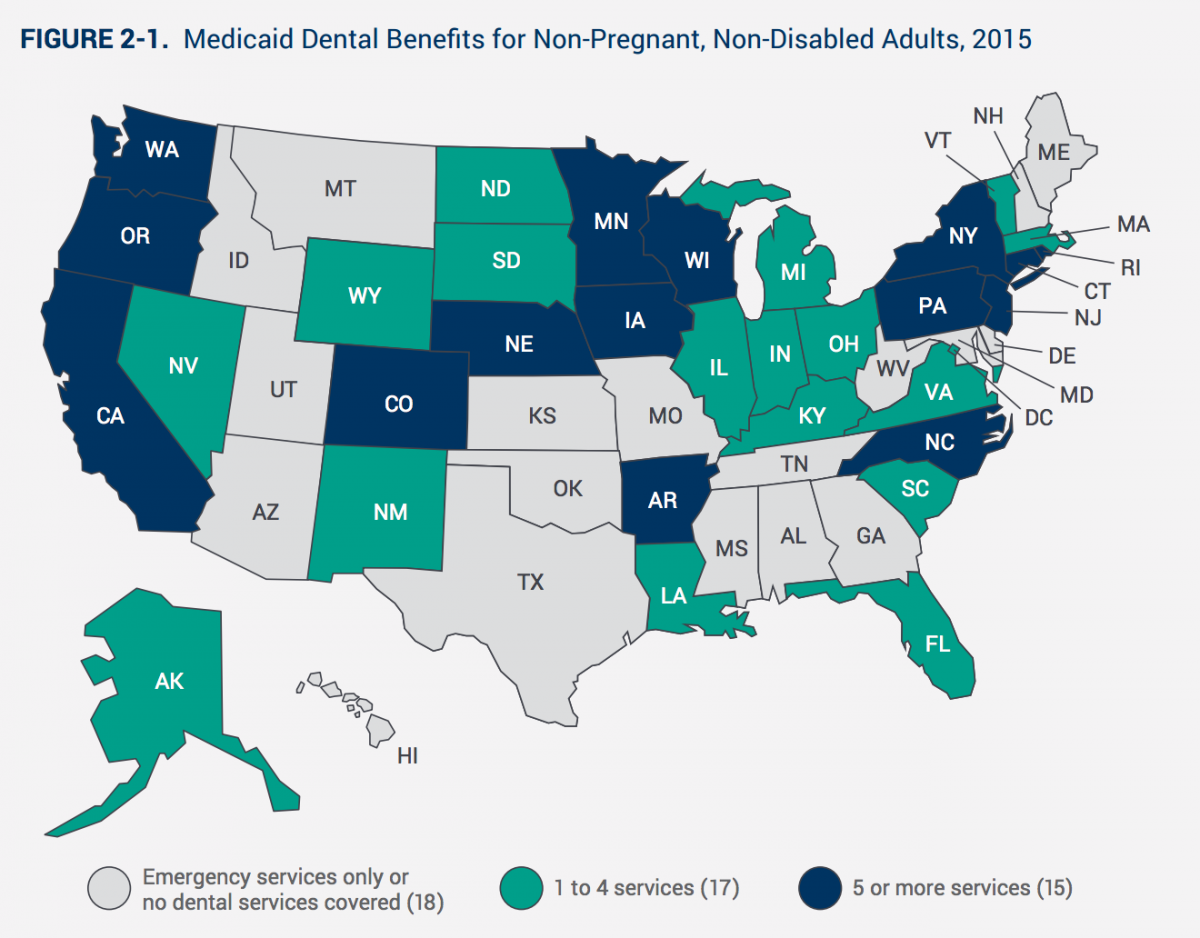
Universal dental access
Federal law does not mandate any minimum requirements for adult dental coverage under Medicaid, and only 27 states cover preventive dental benefits. That’s to the detriment of beneficiaries and also state finances, because end-stage tooth decay may end up costing states in emergency services in the end, MACPAC said.
“Poor oral health is widespread among adults in the United States and especially affects those with low incomes.” Adults with incomes below the poverty level, around $11,700 for a single person, are three times more likely to have untreated cavities than those earning 400 percent of the poverty level, pegged at $47,000.
More than 35 percent of adults above age 65 with incomes below 100 percent of the poverty level have complete tooth loss, compared to just 16 percent of those above 200 percent of the poverty.
“Individuals with a range of chronic conditions are more susceptible to oral disease,” MACPAC said. “Oral disease can also exacerbate chronic disease symptoms. Poor oral health can limit communication, social interaction, and employability.”
While Medicaid must cover dental services for children and youth under age 21, optional coverage for adults varies widely.
Follow Healthcare Finance on Twitter and LinkedIn.
Nineteen state Medicaid programs cover emergency-only adult dental benefits for non-pregnant, non-disabled adults, 26 states cover restorative services, 19 states cover periodontal services, 25 states cover dentures, 25 states covered oral surgery, and 27 cover preventive dental. Nine states have an annual dollar limit on covered dental services.
There are initiatives underway at the state level to expand access to basic dental care in Medicaid, MACPAC said.
These include using mobile clinics and telehealth technologies, increasing the number of providers serving Medicaid enrollees, and funding demonstrations to encourage Medicaid enrollees to increase dental utilization. The National Health Service Corps and some states also offer student loan repayment assistance to dentists who commit to working in high-need, underserved or rural areas, and Minnesota and Alaska amended scope-of-practice laws to allow mid-level dental practitioners to provide dental services.
Here is the full report:
Twitter: @AnthonyBrino

