








































What providers need to know about the bundled payment mandate
Two-percent Medicare price cut will be a challenge, expert states.


In the first year, there is a zero percent discount; the second year, a one percent price cut; and in the third, fourth and fifth years, the two percent price cut goes into effect.
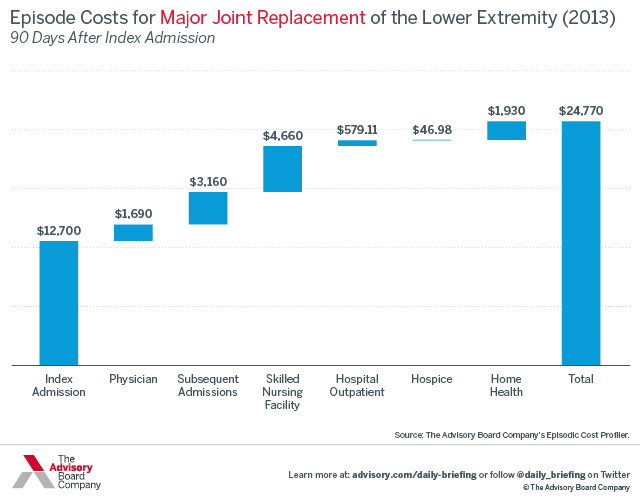
Providers in 75 metro markets are now being required to do what was previously voluntary: bundle Medicare payments for hip and knee surgery from the time of the admission until 90 days post-discharge.
The announcement made Thursday afternoon by Department of Health and Human Services Secretary Sylvia Burwell represents a sizeable shift to providers who were previously taking part in bundled payment programs voluntarily, according to Rob Lazerow, The Advisory Board's expert on the issue.
"With this new program, CMS is making a strong bet on integrated care delivery" Lazerow said, "to make episodes of care of higher quality and more efficient."
One way to create efficiencies is through the program's gainsharing incentives with physicians.
"If an organization can reduce the cost the care, which can mean, either they are reducing the hospital's input cost – either a medical device or an imaging study not paid by Medicare - that can fund gainsharing,” he said. “Or it can be by reducing readmissions or post-acute spend. Any documented savings can be shared with the physicians."
Prior to any financial gains being realized, quality thresholds that must be met.
The program includes a two percent episode price cut, according to Lazerow. Medicare is generating savings by pricing the bundle lower than the sum of the individual service payments.
Providers have a year to plan for the cuts.
In the first year, there is a zero percent discount; the second year, a one percent price cut; and in the third, fourth and fifth years, the two percent price cut goes into effect.
This poses a real challenge to hospitals and health systems, Lazerow said. Providers will need coordinate more effectively with orthopedic surgeons and post-acute care providers to make episodes more efficient and have a more consistent clinical product.
"Providers are going to have to collaborate to reduce costs across that episode to offset that price cut," he said.
This program aligns with incentives from other CMS reforms.
In January, Burwell announced the goal of having 30 percent of Medicare payments tied to alternate payment models by 2016, and 50 percent by 2018.
"I don't think providers were expecting a mandatory bundled payment program," Lazerow said. "This is the first time Medicare has made an alternative payment model mandatory. It's a big wake up call, for those who hoped the transition to new payment models was not as real as it is."

